

62 year old gentleman presents to A&E with chest pain
A good way of thinking of about this is to list the structures are in the location.
A good differential list should always contain common condition and also *ones not to miss (these sohuld be ruled out first).
Asking about the pain is the first key area, think "SOCRATES":
In an acute setting a full history may be inappropriate to obtain before doing an ABCDE assessment. A focused history including past medical / surgical history, medications (including allergies) and family history may be relevant.
Brian Grant is a 62 year old gentleman with pain in his central chest that came on two hours ago. The pain is crushing in nature and radiates to his left arm and his jaw. He feels nauseated with the pain and has some shortness of breath. The pain that he experiences gets worse on exertion. he describes the pain as the worst he has ever felt and expresses a deep concern about his impending doom.
Mr Grant has a history of angina and takes GTN spray for attacks which of late have become increasingly frequent and have begun to trouble him at rest. He also has type two diabetes which was diagnosed 2 years ago and is controlled entirely through diet. He takes no regular medication (except the GTN spray) and has no allergies.
He has no significant family history and lives with his wife who is fit and well, he drinks a moderate amount of alcohol and smokes ten cigarettes per day with 20 pack years under his belt.
Mr Grant is mobile and has previously been in good health other than the comorbidities listed.
Acute Coronary Syndrome (ACS) is a medical emergency where the heart muscle is at risk of damage due to iscaemic heart disease. It is an umbrella term that encompasses unstable angina, non-ST elevation myocardial infarction (NSTEMI) or ST-elevated myocardial infarction (STEMI).
Atheroma is the cause, and it's super-easy to remember the risk factors as they spell 'ATHEROMA' (I wonder if this is how it got its name?):
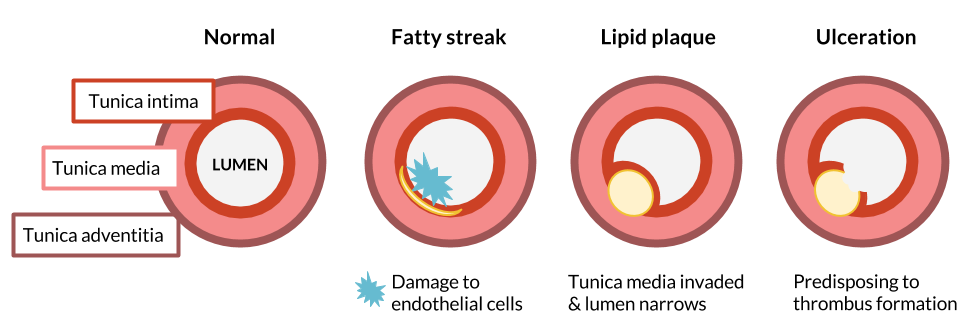
The easiest way to think about atheroma is the 4 layers, 4 stages of development and 4 outcomes.
Always start with the normal when thinking of pathology. The 4 layers of the arterial are:
On a global scale this may cause arteriosclerosis; thick hardening of the arteries due to atheroma.
At medical school we're frequently asked questions by senior doctors like 'A patient comes with a headache - what would you do for them?' or 'A patient has chest pain - what would you do next?'. They are usually asking for something specific but in truth all these questions have only two possible answers:
Which approach to take clearly is dictated by how unwell the patient is, how likely they are to deteriorate or how time sensitive the investigations / management are.
In the case of our patient Mr Grant we've taken a brief history (perhaps too detailed at this stage!) and because we suspect Acute Coronary Syndrome then we should approach this patient with an ABCDE assessment.
Mr Grant is sat up on an A&E trolley, he is pale and short of breath. He still has some chest pain which he scores as 4/10.
Call for help with any acutely unwell patient.
It is important when taking an ABCDE approach to a patient that you correct abnormal findings before reassessing and moving on.

Always ask for "High flow oxygen - 15 litres through a non-rebreather mask" when assessing an acutely unwell patient - you can always reduce it later, i.e. if you are concerned about CO2 retention in COPD patients. It is important in this patient as he has tachynopea and is desaturating.
A chest x-ray would is indicated to look for signs of fluid overload and rule our consolidation / other primary lung pathology. An ABG is a useful investigation for acidosis / alkolisis, quick electrolytes / lactate values and obtaining accurate oxygen and cardon dioxicde levels.
An ECG is critically important for anyone presenting with chest pain. During OSCE stations is may sound obvious to list IV access as part of your interventions, but it is important and a good reminder to mention which bloods and to take cultures if you are concerned about infection.
Pulmonary oedema from acute heart failure is the most likely cause. When part of a coronary artery becomes occluded the tissue supplied by that artery begins to fail.
The heart failure can be due to 3 main things; poor muscle contractility (most common), arryhtmias (from damage to electrical conduction) or valve problems (damage to the papillary muscles).
If part of the muscle in the left ventricle becomes damaged then blood is unable to be pumped effectively from it (and it's ejection fraction falls). The result is that blood backs up in the pulmonary veins leading to pulmonary hypertension, this increased hydrostatic pressure forces fluid from the blood stream into the alveolar spaces in the lungs, impairing gas exchange and leading to desaturation.
.Mr Fence has a set of bloods taken.
| FBC | Value | Normal range |
|---|---|---|
| WBC | 12.84 | 4.5 - 13.5 x 10^9 /L |
| RBC | 4.09 | 4.0 - 6.0 x 10^12 /L |
| Hb | 90 * | 130-150 g/L |
| MCV | 78 * | 90 - 120 fL |
* denotes abnormal result
U&E: NAD
LFT: NAD
Glucose: 4.9 mmol/L (Normal range: 4.4 - 6.1 mmol/L).
The results show a microcytic anaemia (small cells, but normal in number).
Blood loss in the GI tract is either:
The best way to picture anaemia is to think of what goes into making a red blood cell.
Haemoglobin is a protein with iron molecules at it's core. Red blood cells are packed full of haemoglobin, so it makes sense that if iron stores are low then each red blood cell becomes smaller and this manifests as a microcytic anaemia.
Folate and B12 are building blocks of DNA and so are needed to replicate, therefore deficiencies in these will decrease the number of cells, meaning each cell ends up having more haemoglobin and is therefore macrocytic (larger cells).
Urgent 2 week referral for colonoscopy for any of the following:
So which of these does our patient have?
Worryingly he has 3 out of the 5; remember any one of these would merit an endoscopy.
You may find it useful to read the full NICE guidline.
We'd worry more about an inflammatory or infective process, although remember that certain genetic conditions predispose to early onset bowel cancer. Bonus points for naming some.
Inflammatory Bowel Disease (IBD) is a chronic inflammatory autoimmune condition that has two major sub-types: Ulcerative Colitis and Crohn's disease.
The main two symptoms are bleeding per rectum and diarrhoea.
Other symptoms/signs that are included in IBD include:
Note: all these symptoms would have been uncovered with our abdominal history we covered above.
Ulcerative Colitis and Crohn's disease are closely related and both have similar treatments (immunosuppression medication), so why do you need to know the differences? Well because it always comes up in exams.
| Ulcerative Colitis | Crohn's | |
|---|---|---|
| Genetics | DRB-1 | DQ4 DR7 |
| Aetiology | Two peaks: 20-25; 50-60 M=F | One peak: 40-60 F>M |
| Pathology | Starts at rectum, pseudopolyps due to recovering ulcers, mucosa only affected, loss of goblet cells, thin walls | Anywhere from mouth to anus, full thickness granulomatous inflammation, cobblestone appearance with skipped lesions, most common site is terminal ileum |
| Sequelae | Signficant increase in colorectal cancer risk | Fistulas, strictures and bowel obstruction, abscess, mile increase in colorectal cancer |
Mr Fence went to hospital for a colonoscopy which revealed several polyps in the ascending and transverse colon and a large mass in the caecum of the colon. This was biopsied and found to be malignant.
Bowel polyps are small growths on the inner lining of the colon (large bowel) or rectum. They are common, affecting 15-20% of the UK population, and don't usually cause symptoms.
Bowel polyps are not usually cancerous, although if they're discovered they'll need to be removed, as some will eventually turn into cancer if left untreated.
You can read more about polyps at NHS choices.
It is important to understand the link between dysplasia and malignancy.
Histology of a polyp on a stalk (pedunculated) areas 1, 2 &3 from bottom up representing normal dysplastic and neoplastic regions.

After Mr Fence had his colonoscopy he was informed that it was a cancerous growth. The fact that Mr Fence's cancer was confined to his colon (that it had not metastasised), him being a fit and healthy man for his age, it was advised that he have surgery to remove the caecum, the ascending colon and the hepatic flexure.
To learn more about types of operations done please visit: Cancer Research UK.
Wow! You made it all the way to the end. These are the objectives you will have picked up along the way.