

73 year old presents with general tiredness
A differential diagnosis for tiredness is quite broad, therefore using a framework may help in adding structure and uncovering your knowledge.
We'll use the surgical sieve 'VINDICATE':
Remember the functional and psychiatric conditions that may present as tiredness such as depression and chronic fatigue syndrome.
Obviously because this case sits within a gastrointestinal section we'll focus on those parts of the history, but patients don't present as easily as this!
When taking a GI history it can be thought of as:
Robert Fence is a 73 year old retired builder who has been growing progressively more tired for the last 6 months. He has reported no other symptoms of note apart from an occasional discomfort in his abdomen. He has not been bloated nor has he had any bloody stool, and has never had a positive Faecal Occult Blood Test. He has noticed his stools have become looser in the last 4 months.
He has lost weight of 3.3kg without changing his diet or exercise regime, he is not overly thirsty and doesn't report any change to his skin colour.
Mr Fence has no past medical history of note and has self reportedly been in good health for as long as he can remember. He has no allergies and is on no regular medication. he is an ex-smoker of 10 pack years and drinks moderate amounts of alcohol. He lives at home with his wife and is fully independant. He is concerned about the progressive nature of his tiredness.
Again when thinking of a differential diagnosis try and use a framework to help pin your ideas to.
When dealing with tube-like structures one technique is to think of causes anatomically; in the lumen, in the bowel wall, outside the bowel wall.
Different pathological processes affect different layers, so make sure you're familiar with them as you may be asked by an inquisitive consultant on a ward round.
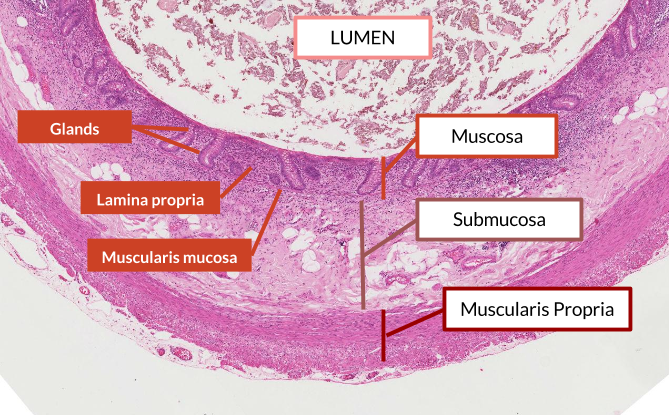
The normal layers of the GI tract can be difficult to remember, so we've created a short video to talk you through.
Below is how the layers appear under a microscope.
General inspection: Patient comfortable at rest.
Obs:
Abdominal examination: Mr Fence had a pale conjunctiva. Abdomen was soft, non-tender with no mass and no organomegaly. Digital rectal examination was normal.
A very basic routine for any examination would be general inspection, hands, face and finally the system you are examining. Using this approach you may find the following in someone with anaemia:

Mr Fence has a set of bloods taken.
| FBC | Value | Normal range |
|---|---|---|
| WBC | 12.84 | 4.5 - 13.5 x 10^9 /L |
| RBC | 4.09 | 4.0 - 6.0 x 10^12 /L |
| Hb | 90 * | 130-150 g/L |
| MCV | 78 * | 90 - 120 fL |
* denotes abnormal result
U&E: NAD
LFT: NAD
Glucose: 4.9 mmol/L (Normal range: 4.4 - 6.1 mmol/L).
The results show a microcytic anaemia (small cells, but normal in number).
Blood loss in the GI tract is either:
The best way to picture anaemia is to think of what goes into making a red blood cell.
Haemoglobin is a protein with iron molecules at it's core. Red blood cells are packed full of haemoglobin, so it makes sense that if iron stores are low then each red blood cell becomes smaller and this manifests as a microcytic anaemia.
Folate and B12 are building blocks of DNA and so are needed to replicate, therefore deficiencies in these will decrease the number of cells, meaning each cell ends up having more haemoglobin and is therefore macrocytic (larger cells).
Urgent 2 week referral for colonoscopy for any of the following:
So which of these does our patient have?
Worryingly he has 3 out of the 5; remember any one of these would merit an endoscopy.
You may find it useful to read the full NICE guidline.
We'd worry more about an inflammatory or infective process, although remember that certain genetic conditions predispose to early onset bowel cancer. Bonus points for naming some.
Inflammatory Bowel Disease (IBD) is a chronic inflammatory autoimmune condition that has two major sub-types: Ulcerative Colitis and Crohn's disease.
The main two symptoms are bleeding per rectum and diarrhoea.
Other symptoms/signs that are included in IBD include:
Note: all these symptoms would have been uncovered with our abdominal history we covered above.
Ulcerative Colitis and Crohn's disease are closely related and both have similar treatments (immunosuppression medication), so why do you need to know the differences? Well because it always comes up in exams.
| Ulcerative Colitis | Crohn's | |
|---|---|---|
| Genetics | DRB-1 | DQ4 DR7 |
| Aetiology | Two peaks: 20-25; 50-60 M=F | One peak: 40-60 F>M |
| Pathology | Starts at rectum, pseudopolyps due to recovering ulcers, mucosa only affected, loss of goblet cells, thin walls | Anywhere from mouth to anus, full thickness granulomatous inflammation, cobblestone appearance with skipped lesions, most common site is terminal ileum |
| Sequelae | Signficant increase in colorectal cancer risk | Fistulas, strictures and bowel obstruction, abscess, mile increase in colorectal cancer |
Mr Fence went to hospital for a colonoscopy which revealed several polyps in the ascending and transverse colon and a large mass in the caecum of the colon. This was biopsied and found to be malignant.
Bowel polyps are small growths on the inner lining of the colon (large bowel) or rectum. They are common, affecting 15-20% of the UK population, and don't usually cause symptoms.
Bowel polyps are not usually cancerous, although if they're discovered they'll need to be removed, as some will eventually turn into cancer if left untreated.
You can read more about polyps at NHS choices.
It is important to understand the link between dysplasia and malignancy.
Histology of a polyp on a stalk (pedunculated) areas 1, 2 &3 from bottom up representing normal dysplastic and neoplastic regions.

After Mr Fence had his colonoscopy he was informed that it was a cancerous growth. The fact that Mr Fence's cancer was confined to his colon (that it had not metastasised), him being a fit and healthy man for his age, it was advised that he have surgery to remove the caecum, the ascending colon and the hepatic flexure.
To learn more about types of operations done please visit: Cancer Research UK.
Wow! You made it all the way to the end. These are the objectives you will have picked up along the way.